An Axillary Temperature Reading Is Recorded as Follows 102.2
Vital Signs
Learning Objectives
Vocabulary
apnea (ap′-nee-uh) Absenteeism or abeyance of animate.
arrhythmia An abnormality or irregularity in the center rhythm.
arteriosclerosis (ar-ter′-ee-o-scler-o-sis) Thickening, decreased elasticity, and calcification of arterial walls.
bounding Term used to describe a pulse that feels total because of increased power of cardiac contraction or as a result of increased blood volume.
bradycardia (brad-i-kahr′-dee-uh) A slow heartbeat; a pulse below 60 beats per minute.
bradypnea (brad-ip-nee′-uh) Respirations that are regular in rhythm but slower than normal in rate.
cerumen (see-room′-men) A waxy secretion in the ear canal; normally called ear wax.
chronic obstructive pulmonary disease (COPD) A progressive, irreversible lung condition that results in diminished lung capacity.
diurnal (die-ur′-nl) rhythm Design of action or behavior that follows a 24-hour interval-night cycle.
dyspnea (disp-nee′-uh) Hard or painful animate.
essential hypertension Elevated blood force per unit area of unknown cause that develops for no apparent reason; sometimes called primary hypertension.
febrile (feb′-ril) Pertaining to an elevated body temperature.
homeostasis Internal adaptation and change in response to ecology factors; multiple functions that attempt to continue the body'southward functions in residual.
hyperpnea (hahy-per-nee′-uh) An increase in the depth of breathing.
hypertension High claret pressure.
hyperventilation Abnormally prolonged and deep breathing, usually associated with acute anxiety or emotional tension.
hypotension Claret pressure that is below normal (systolic force per unit area below 90 mm Hg and diastolic pressure beneath 50 mm Hg).
intermittent pulse A pulse in which beats occasionally are skipped.
orthopnea (or-thop′-nee-uh) Condition in which an individual must sit or stand to exhale comfortably.
orthostatic (postural) hypotension A temporary fall in blood pressure when a person rapidly changes from a recumbent position to a standing position.
otitis externa Inflammation or infection of the external auditory canal (swimmer'southward ear).
peripheral (puh-rif′-er-uhl) Term that refers to an area exterior of or abroad from an organ or structure.
pulse deficit Condition in which the radial pulse is less than the apical pulse; may indicate a peripheral vascular abnormality.
pulse pressure The difference between systolic and diastolic blood pressures (30 to 50 mm Hg is considered normal).
pyrexia (pi-rek′-see-uh) Febrile condition or fever.
rales Abnormal or crackling jiff sounds during inspiration.
rhonchi (ron′-ki) Aberrant rumbling sounds on expiration that indicate airway obstruction by thick secretions or spasms.
secondary hypertension Elevated blood pressure level resulting from another condition, typically kidney affliction.
sinus arrhythmia Irregular heartbeat that originates in the sinoatrial node (pacemaker).
spirometer Instrument that measures the volume of air inhaled and exhaled.
stertorous (stuh-tuh′-rus) Term that describes a strenuous respiratory endeavor marked by a snoring sound.
syncope (sing′-kuh-pee) Fainting; a brief lapse in consciousness.
tachycardia (tak-i-kahr′-dee-uh) A rapid but regular heart rate; one that exceeds 100 beats per minute.
tachypnea (tak-ip-nee′-uh) Condition marked by rapid, shallow respirations.
thready Term that describes a pulse that is scarcely perceptible.
wheezing A loftier-pitched sound heard on expiration; indicates obstruction or narrowing of respiratory passages.
Scenario
Dr. Susan Xu is a fellow member of a multiphysician primary care practice. Each doctor in the practice has a medical banana who works directly with him or her. Carlos Ricci, CMA (AAMA), is Dr. Xu'due south banana. Carlos graduated from a medical assistant program three years ago and enjoys the diverseness of patients seen in Dr. Xu's practice. I of Carlos' main responsibilities is to accurately measure and record each patient'south vital signs before the patient is seen by Dr. Xu.
While studying this chapter, think about the post-obit questions:
Measurement of vital signs is an important aspect of virtually every patient visit to the medical office. These signs are the human body's indicators of internal homeostasis and the patient's full general state of health. Because medical administration are chiefly responsible for obtaining these measurements, it is imperative that they have confidence in the theoretic and practical applications of vital sign measurement. A medical assistant who understands the principles of and the reasons for these measurements becomes a valuable asset to any medical part.
Accuracy is essential. A change in ane or more of the patient's vital signs may indicate a change in full general health. Variations may advise the presence or disappearance of a disease procedure and therefore may lead to alteration of the handling program. Although the medical banana obtains vital signs routinely, it is a task that requires consistent attention to accuracy and detail. These findings are crucial to a correct diagnosis, and vital signs should never be measured with indifference or casualness. In addition to performing accurate measurement, intendance must exist taken when charting the findings on the patient's medical tape.
Vital signs are the patient's temperature, pulse, respiration, and blood pressure. These four signs are abbreviated TPR and BP and may be referred to equally central signs. The medical assistant must empathise the significance of the vital signs and must measure and tape them accurately. Anthropometric measurements are not considered vital signs just usually are obtained at the same time every bit vital signs. These measurements include height, weight, body mass index (BMI), and other body measurements, such every bit fat composition and an infant's head circumference.
Factors That May Influence Vital Signs
Vital signs are influenced by many factors, both physical and emotional. A patient may have drunk a hot or cold potable just before the exam or may exist aroused or fearful well-nigh what the physician may find. For example, consider that a patient has been asked to return to have a repeat Papanicolaou (Pap) smear because the get-go one showed the presence of suspicious cells. The medical assistant measures the patient'south blood pressure and finds it significantly elevated compared with previous readings. The patient may be anxious and apprehensive about the test results, and the elevated claret pressure readings reflect her anxiety.
What temperature reading might exist expected in a patient who could not find a parking place and had to walk four blocks to the role, knowing he would exist tardily for his date? If yous said it would be elevated, you are correct. Certainly, this patient'south metabolism would increment considering of the concrete practise, and as a result, his temperature would be elevated, along with his pulse, respirations, and blood force per unit area.
For one reason or some other, many patients are apprehensive during an office visit. These emotions may modify vital signs, and the medical assistant must aid the patient relax before taking any readings. Measurements sometimes must be obtained a second time, after the patient is calmer or more comfortable. For a better picture of the patient's vital signs, the medical assistant may exist asked to record the vital signs twice: at the kickoff of the visit and just earlier the patient leaves the function.
Temperature
Physiology
Torso temperature is defined as the balance between estrus lost and heat produced past the trunk. It is measured in degrees Fahrenheit (F) or degrees Celsius (C). The process of chemical and physical change in the torso that produces estrus is called metabolism. Body temperature is a result of this process. The core body temperature is maintained within a normal range by the thermoregulatory eye in the hypothalamus. The average trunk temperature varies from person to person and is dissimilar in each person at different times throughout the 24-hour interval. In a healthy developed, this diurnal rhythm varies from 97.6° F to 99° F (36.4° C to 37.3° C); the average daily temperature is 98.6° F (36.8° C). Body temperature is lowest in the morning and highest in the late afternoon. Factors that may affect body temperature include the post-obit:
In illness, an private'south metabolic activity is increased; this causes an increase in internal heat product, which in turn raises the torso temperature. The increment in body temperature is thought to be the body's defensive reaction because rut inhibits the growth of some leaner and viruses.
When a fever is present, superficial blood vessels (those about the surface of the skin) constrict. The small-scale papillary muscles at the base of operations of hair follicles likewise constrict, creating goose bumps. Chills and shivering may follow, producing internal heat. As this process repeats itself, more heat is produced, and the body temperature becomes elevated or rises above the normal range. When more than oestrus is lost than is produced, the opposite effect occurs, and body temperature drops below normal range.
Fever
Infection, either bacterial or viral, is the most common cause of fever in both children and adults.
Infants do not usually develop febrile illnesses during the first iii months of life; if 1 is present, it usually is very serious. Yet, fever, or pyrexia, is very common in young children and accounts for an estimated 26% of office visits. Fevers are classified according to the 24-hour pattern they follow. The three near common patterns are:
Variation from the patient'southward average trunk temperature range may exist the first alarm of an illness or a change in the patient's current condition. Patients with fever usually have loss of appetite (anorexia), headache, thirst, flushed face, hot skin, and full general malaise. Some patients experience an astute onset of chills and shivering followed past an increase in body temperature. A serious possible complication in immature children with high fevers is a febrile seizure. Medication to reduce the fever, or antipyretic drugs (e.grand., Tylenol), should exist taken as instructed to prevent dangerous spikes in temperature. Age-related normal values for temperature readings are shown in Tabular array 31-1.
Temperature Readings
A clinical thermometer is used to measure body temperature. It is calibrated in the Fahrenheit or the Celsius scale. The Fahrenheit scale is used most often in the United States, but hospitals and many convalescent care settings apply the Celsius scale. The formulas for conversion from one system to the other are as follows:
For case, if an infant'due south temperature is measured at 101° F, the Celsius conversion would be:
If the ambulatory care setting where you work uses a Celsius thermometer, patients may inquire you what the temperature is in Fahrenheit degrees because that is the scale they sympathise. If the facility does non have a conversion chart available, you volition need to catechumen the temperature mathematically. For example, if an infant'due south temperature is 39° C, what is the Fahrenheit reading?

Several types of thermometers and several dissimilar methods tin be used to accept temperature readings. A digital thermometer is placed under the tongue, in the armpit, or rectally; a tympanic thermometer is inserted into the ear; and a temporal artery scanner is moved beyond the forehead. Average temperature values for adults at the four nigh mutual sites are shown in Tabular array 31-two.
Axillary temperatures are approximately 1° F (0.6° C) lower than accurate oral readings because axillary readings are not taken in an enclosed body cavity. When taken correctly, the tympanic (ear) temperature is an authentic measure because it records the temperature of the claret closest to the hypothalamus. Yet, recent research on the newest device for obtaining temperature, the temporal artery (TA) thermometer, indicates that this method is more than accurate than tympanic measurement for identifying elevated temperatures in infants. Pediatricians, therefore, may prefer TA temperatures in infants suspected of having a fever. The TA thermometer likewise records accurate temperature readings in all historic period groups of patients. The tympanic method nevertheless is considered a fast, accurate, and noninvasive manner of recording temperatures for older children and adults.
When obtaining an oral temperature, you practise not have to indicate the site when documenting the reading in the patient's chart. Nevertheless, you should write (T) for tympanic, (A) for axillary, or (TA) for temporal artery readings after recording the temperature to analyze that an alternative site was used. Oral temperature cannot exist measured accurately in young children considering the technique requires patients to agree the thermometer under the tongue and keep the mouth airtight. To accept an infant's temperature rectally, lubricate the probe tip, hold the infant securely with the legs elevated, and insert the probe approximately ½ inch; hold the probe advisedly throughout the procedure to prevent rectal damage. However, pediatricians may prefer that infants' temperatures be taken with a temporal thermometer because information technology is more comfortable for the baby, is less invasive, and eliminates the possible complexity of a perforated rectum.
For patients older than 3 years and for those unable to hold a thermometer properly in their mouth during the process, a tympanic or temporal thermometer can be used; if not, a less accurate axillary temperature tin can be obtained.
Types of Thermometers and Their Uses
Digital Thermometer
Digital thermometers are battery operated and are available in both Fahrenheit and Celsius scales. Disposable covers fit snugly over the probes and are easily and quickly removed by pushing in the colored finish of the probe. The instrument sounds a beep when the procedure is completed (10 to 60 seconds), and the reading appears on a light-emitting diode (LED) screen on the face of the instrument (Procedure 31-one). Because the simply part of the instrument that comes in contact with the patient is the probe, which is sheathed, the run a risk of cross-infection is profoundly reduced (Figure 31-ane). Another blazon of digital thermometer resembles the erstwhile mercury thermometers that the Occupational Safety and Health Assistants (OSHA) no longer allows clinicians to use in healthcare facilities. These thermometers take a digital screen on which the temperature is read and should always be covered by a disposable sheath.
Temperature should not be taken orally if the patient recently has had something hot or cold to eat or drink or has just smoked, because these factors may artificially alter the patient's temperature. In addition, the patient must be able to hold the thermometer under the tongue with the lips tightly sealed around the probe of an authentic oral reading is to exist obtained.
Tympanic Thermometer
The tympanic membrane of the ear can be used for quick, accurate, and safe cess of a patient'southward temperature. It shares the blood supply that reaches the hypothalamus, which is the encephalon'due south temperature regulator. The ear canal is a protected cavity, and so aural temperature is non affected by factors such equally an open mouth, hot or common cold drinks, or even a stuffy nose, which would prevent a patient from keeping the mouth closed during the process. In addition, the covered probe is designed to bounce an infrared signal off the eardrum without touching it, and so the take a chance of spreading communicable diseases during temperature measurement is greatly reduced.
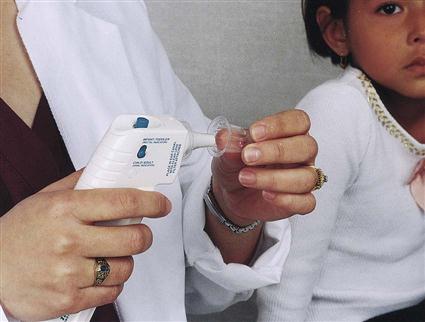
The tympanic measurement organization consists of a handheld processor unit of measurement equipped with a tympanic probe, which is covered with a disposable speculum for utilise (Figure 31-two).
When the probe is placed into the ear canal, it gently seals the external opening of the canal, and the infrared energy emitted by the tympanic membrane is gathered. This signal is digitized by the processor unit of measurement and is shown on the display screen. Accurate readings are obtained in less than two seconds (Procedure 31-2). Both the speed of the tympanic thermometer and the comfort it affords the patient have greatly influenced its popularity. Still, this unit should not be used (ane) if the patient has bilateral otitis externa, considering the procedure would be uncomfortable for the patient, and (two) if impacted cerumen is present in both ears, considering the reading may be inaccurate.
Procedure 31-2
Obtain Vital Signs
Obtain an Audible Temperature Using the Tympanic Thermometer
GOAL:To accurately determine and record a patient's temperature using a tympanic thermometer.
EQUIPMENT and SUPPLIES
Procedural Steps
i. Sanitize your hands.
PURPOSE: To ensure infection control.
2. Get together the necessary equipment and supplies.
three. Identify your patient and explain the process.
PURPOSE: Identification of the patient prevents errors, and explanations are a ways of gaining implied consent and patient cooperation.
four. Place a disposable embrace on the probe (Effigy 1).
PURPOSE: To ensure a clean surface and forbid cross-contamination.
5. Follow the package directions to start the thermometer.
6. Insert the probe into the ear canal far enough to seal the opening. Do not apply pressure (Figure two). For children younger than age iii, gently pull the earlobe down and back; for patients older than age 3, gently pull the superlative of the ear upwardly and back.

PURPOSE: The external ear must exist pulled gently to open the external auditory canal and expose the tympanic membrane for an accurate reading.
7. Printing the push on the probe as directed. The temperature will appear on the display screen in ane to two seconds.
8. Remove the probe, note the reading (Figure iii), and discard the probe comprehend into a biohazard container without touching it.

PURPOSE: The probe cover is contaminated and must exist discarded in a biohazard waste material container.
9. Sanitize your hands and disinfect the equipment if indicated.
PURPOSE: To ensure infection control.
10. Record the temperature results (e.1000., T = 98.vi° F [T]) in the patient'southward medical record.
PURPOSE: Procedures that are non recorded are considered not washed.
3/xxx/XX 2:twenty PM T 101.2° F (T) — — — — — — — C. Ricci, CMA (AAMA) ____________________________
Temporal Avenue Scanner
The temporal artery scanner uses an infrared beam to assess the temperature of the claret flowing through the temporal avenue of the lateral forehead, where the artery lies nigh 1 mm below the pare (Effigy 31-iii). Considering the artery is so close to the skin, it provides good surface heat conduction, allowing the thermometer to obtain a fast, accurate, and noninvasive measurement of the body temperature.
To perform the process, place the probe in the eye of the forehead, halfway between the eyebrows and the hairline. Bangs should be pushed back off the forehead (this method cannot exist used if bandages cover the area). Depress the button on the scanner and gently stroke the probe across the forehead toward the hairline (at the temples), keeping the probe flat on the patient's skin. As the scanner moves across the forehead, repeated temperature measurements are taken and the highest measurement is recorded; keeping the push depressed, lift the scanner from the temporal area and lightly place the probe behind the earlobe. Release the button and remove the probe. Recording an accurate temperature takes about iii seconds (Procedure 31-3).
Procedure 31-3
Obtain Vital Signs
Obtain a Temporal Artery Temperature
GOAL:To accurately determine and tape a patient's temperature using a temporal artery scanner.
EQUIPMENT and SUPPLIES
Procedural Steps
1. Sanitize your hands.
PURPOSE: To ensure infection control.
two. Get together the necessary equipment and supplies.
iii. Innovate yourself, identify your patient, and explain the procedure.
PURPOSE: Identification of the patient prevents errors, and explanations are a means of gaining implied consent and patient cooperation.
four. Remove the protective cap on the probe. The probe tin be cleaned by lightly wiping the surface with an booze swab.
5. Push the patient's hair up off of the forehead to betrayal the site. Gently identify the probe on the patient'southward brow, halfway between the eyebrows and the hairline.
PURPOSE: This places the probe direct over the temporal artery.
half-dozen. Depress and concur the SCAN push button and lightly glide the probe sideways across the patient'due south forehead to the hairline simply to a higher place the ear (Effigy i). Equally you move the sensor across the forehead, you will hear a beep, and a red lite volition flash.

PURPOSE: This verifies that the scanner is recording temperatures as it moves beyond the surface of the temporal artery.
7. Go along the button depressed, lift the thermometer, and place the probe on the upper neck behind the ear lobe (Figure ii). The thermometer may proceed to beep, indicating that the temperature is ascension.

PURPOSE: To continue scanning of the temporal artery until the highest temperature is recorded on the thermometer.
viii. When scanning is complete, release the button and lift the probe. Note the temperature recorded on the digital display. The scanner automatically turns off 15 to 30 seconds subsequently release of the button.
9. Disinfect the thermometer if indicated and supersede the protective cap.
PURPOSE: To ensure infection control.
10. Sanitize your hands.
eleven. Record the temperature results (e.g., T = 101.6° F [TA]) in the patient's medical record.
PURPOSE: Procedures that are non recorded are considered not done.
Axillary Thermometer
Studies signal that axillary temperatures are accurate when performed correctly. Axillary temperatures take more than time to register the correct body temperature, just the method is safe, simple, and like shooting fish in a barrel to perform (Procedure 31-4). Axillary temperatures are taken with a digital thermometer, which is placed into the axillary fold. If the digital thermometer has more than one probe, the oral (blue) probe with a disposable probe cover should be used. Because tympanic and temporal thermometers are relatively expensive, the axillary method may be a viable way for parents of young children to get accurate temperature readings at abode. Nonetheless, parents should be enlightened that the axillary temperature may be every bit much equally one degree less than the child'southward actual cadre temperature.
slaughterwiforece.blogspot.com
Source: https://nursekey.com/vital-signs-4/
0 Response to "An Axillary Temperature Reading Is Recorded as Follows 102.2"
Post a Comment